

Background
Hyperfibrinolysis is a pathologic state of fibrin(ogen) degradation which can be observed in disseminated intravascular cogulation (DIC), post-partum hemorrhage, trauma, or liver transplant settings. Hyperfibrinolysis is associated with bleeding, transfusion, and adverse patient outcomes (Pommerening et al. J Am Coll Surg 2014. 219: 1157). Rapid administration of antifibrinolytics has been demonstrated to significantly improve mortality (Ker et al. Cochrane Database of Systematic Reviews 2015, Issue 5). Thromboelastography (TEG) and rotational thromboelastometry (ROTEM) are viscoelastic testing methods which allow rapid assessment of many aspects of hemostasis including hyperfibrinolysis. TEG/ROTEM have largely replaced euglobulin clot lysis as laboratory methods of diagnosing hyperfibrinolysis. However, the sensitivity and specificity of TEG/ROTEM abnormalities for diagnosis of hyperfibrinolysis is not well-described.
Methods
TEG 5000 (CK alone, CK/CKH, or CK/CRT/CFF packages) were ordered by clinicians based on clinical need. TEG 6S (Global Hemostasis cartridge) is also performed at our institution but is not included due to lack of lysis data in the FDA-approved reportable parameters.
All TEG testing performed over a 17.75 month span (March 2018 to October 2019) was reviewed for hyperfibrinolysis, defined as LY30 >5% based on locally validated reference range. Patient demography, other lab data, management including blood product use and antifibrinolytics, and survival were reviewed.
Results
19532 test traces across 9952 sample accessions were performed from 2076 unique patients. Of these, 84 traces (0.85%) across 72 accessions (0.72%) from 56 patients (2.70%) exhibited LY30 >5%. Of TEG runs that showed abnormal lysis that were run with multiple reagents, 7.6% showed elevated lysis in 2+ traces, while 92.4% showed elevated lysis in just one trace.
The most common clinical contexts for elevated LY30 were ECMO use (N=18), post-partum hemorrhage (N=15), and trauma (N=12). Four trauma patients demonstrated a distinct "black diamond" trace pattern with high LY30 and return of curve to baseline, all of whom died during admission. Patients on ECMO demonstrated a trace which scalloped after achievement of maximal amplitude ("secondary hyperfibrinolysis") and may not represent true fibrinolysis.
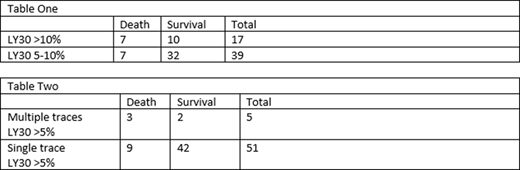
Admission survival was decreased in patients with LY30 >10% (41.2%) as compared to LY30 5-10% (18.4%); this was not significant by Fisher's exact test (Table One). All deaths following within 36 hours of testing showed LY30 >10%. Positive predictive value of LY30>10% for admission mortality (relative to LY30 5-10%) was 41%, negative predictive was 82%.
Survival was decreased in patients with LY >5% in multiple traces (40%) as compared to patients with LY >5% in only one trace (21.4%) (Table Two); this was also not significant by Fisher's exact test. Positive predictive value of multiple traces with LY30>5% for admission mortality (relative to single trace) was 60%, negative predictive value was 82%.
Patients with LY30 >10% (as compared to LY30 between 5-10%) were more likely to undergo subsequent massive transfusion (41.2% vs 23.7%) or receive cryoprecipitate (17.4% vs 7.7%). Antifibrinolytics were only administered in 3 postpartum hemorrhage patients.
Discussion
In this retrospective study, we cannot comment on the analytical sensitivity or specificity of TEG hyperfibrinolysis detection relative to a different methodology. However, we have used the outcomes of patients with LY30 abnormalities to estimate clinical predictive vaules. LY30 >5% is a nonspecific cutoff for diagnosis of hyperfibrinolysis. Absent a gold-standard method, we suggest a cutoff of LY30 >10% or LY30 abnormality in multiple TEG traces as a more specific indicator of clinically significant hyperfibrinolysis. Absence of such degrees of LY30 abnormality has an 82% NPV for death during admission.
Wool:STAGO: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal